Trial Short Case 3 April 2022
Case Summary
76 yo male
SOB while sitting on couch on background increasing SOBOE.
Negative troponins, underwent angiogram given risk factors
Could walk 4-5Km/day with breathlessness on hills, hill tolerance slowly declining past 12 months. Now struggles to walk 10 minutes on flat.
referred for consideration of surgical revascularization
Background
IHD – prev PCI to LAD, Lcx and RCA
AF – anticoagulated for 6 years
COPD
FEV1 1.84L (64% predicted), FVC 2.76L (75% predicted), FEV1/FVC 0.66 (83% pred)
DLCO 68% predicted
Anxiety/depression
Chronic kidney disease: Cr 130umol (eGFR 46)
T2DM: HbA1c 7
Medications
Aspirin 100mg
Rivaroxaban 10mg BD
Rosuvastatin 20mg
Fluticasone + Salmeterol 250/25 mcg BD
Citalopram 20mg
Olmisartan 40mg / hydrochlorothiazide 25mg
Gliclazide 30mg
Linagliptin 5mg
Examination
78kg, 172cm, BMI 26.37
HR 90 irregular
BP 118/76
JVP 5cm
Nil peripheral oedema
Fixed, split second heart sound, no murmurs
Chest – clear
No varicose veins, Allens brisk 2 sec bilaterally, no chest scars or deformities
Investigations
HB 118, Plt 201, INR 1.6
K 3.8 , Cr 138
Albumin 36
HbA1C 7.1
Serology – all negative
ECG
AF
LBBB
CXR
NAD
CT chest (non-contrast)
Smooth interstitial thickening consistent with mild interstitial oedema
No emphysema or bronchiectasis
TOE
3cm sinus venosus ASD
Anomalous right upper lobe pulmonary vein draining to SVC/RA junction
3 pulmonary veins draining into LA - well visualized
Remainder of exam as per TTE
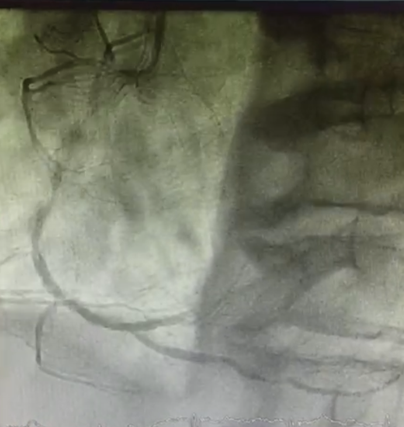
Angiogram



TTE


Right Heart Cath



Questions:
What are the potential causes of pulmonary hypertension in this patient? What features of the investigations included make you think one is more or less likely than others. What, if any, further investigations would you consider?
Briefly discuss embryological basis for a sinus venosus ASD and its anatomical location? What, if any, are the other pertinent cardiac lesions associated with a sinus venosus ASD?
What is your surgical approach to this patient?