Trial Short Case 1April 2022
Case Summary
A 59-year-old male underwent primary investigation for new onset atrial fibrillation.
Worsening SOB with activity.
NYHA II
The patient had been anticoagulated by his primary physician. Initial exam and primary screening investigations did not demonstrate any known causes for atrial fibrillation. The patient progressed to a trans thoracic echocardiogram.
Background
Bipolar affective disorder
HTN
Hypercholesterolaemia
T2DM
Testicular Cancer - Orchidectomy and Chemotherapy
GORD
Non smoker
nil EtOH
BMI normal
nil family history of arrhythmia
nil OSA
Medications
Apixaban 5mg BD
Perindopril 2.5mg
Metformin XR 1g
Examination
90kg, 175cm
HR 92 bpm irregular
BP 145/75
JVP not elevated
Warm peripheries, strong irregular radial pulse
No carotid bruits
HS 1+2 + nil added
Chest - equal air entry, no creps/wheeze
Calves soft not tender
Nil peripheral oedema
Nil varicose veins
Thyroid exam unremarkable
Investigations
Bloods
CBE: Hb 133 / WCC 5.25 / Plt 221
EUC: Na 140/ K 4.3 / Creat 72
LFT: unremarkable
Coagulation Profile: INR 1.0 / APTT 32
Troponin 6
CK 116
HbA1c 7.1%
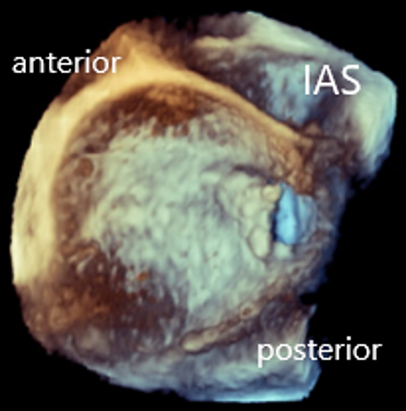
TTE:
A divided left atrium, separating the pulmonary veins from the mitral orifice. Nil thrombus in the left atrial appendage. Nil valvular pathology The left atrium was dilated (81ml/m2) and the interatrial septum was intact. LV function normal – 60%
Stress TTE:
Increase in the gradient across the membrane opening from 4mmHg to 14mmHg, and no increase in right heart pressures.
TOE
The right and left upper pulmonary veins drained into the superior segment of the left atrium, and majority of blood flowed across a single posterior opening (1.5cm2) in the membrane.


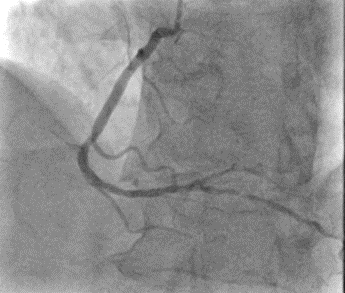
Angiogram
•Left Main Coronary Artery: Patient with minor non critical atheroma
•Left Anterior Descending Coronary Artery: Patient with minor non critical atheroma
•Circumflex Coronary Artery: Co-dominant artery – patent with minor non critical atheroma
•Left Ventricle: EDP 10mmHg, no significant aortic pullback gradient
•Right Coronary Artery: Co – dominant artery, right PDA is a moderate vessel with severe 80% mid vessel stenosis


Right Heart Cath

Questions:
What is the primary pathology in this patient? Where does this anomaly occur and what is the cause?
Explain the results of this patient’s investigations, your interpretation explain your reasoning for the new onset atrial fibrillation?
What is the evidence for surgical intervention on this gentleman’s atrial fibrillation?
After concomitant left atrial appendage closure, the patient is requesting cessation of their blood thinning agents. What is the current evidence for this?